Outbreak at a glance
As of 8 July 2022, 35 countries in five WHO Regions have reported 1010 probable cases of severe acute hepatitis of unknown aetiology in children, which fulfill the WHO case definition, including 22 deaths. Since the previous Disease Outbreak News published on 24 June 2022, 90 new probable cases and four additional deaths have been reported to WHO. Additionally, two new countries, Luxembourg and Costa Rica, have reported probable cases.
WHO has launched a global survey with an aim to estimate the incidence of severe acute hepatitis of unknown aetiology in 2022 compared to the previous five years, to understand where cases and liver transplants are occurring at higher-than-expected rates.
This Disease Outbreak News provides updates on the epidemiology of the outbreak, as well as updates on the response to this event, including the launch of the clinical case report form on the WHO Global Clinical Platform, and updates on Infection Prevention and Control (IPC) and risk communication and community engagement (RCCE).
Description of the outbreak
Between 5 April (when the outbreak was initially detected) and 8 July 2022, 35 countries in five WHO Regions have reported 1010 probable cases (Figure 1) and 22 deaths. These include new and retrospectively identified cases since 1 October 2021, which fit the WHO case definition as stated below. There are three additional countries that have reported cases which are pending classification and are not included in the cumulative probable case count. Of the probable cases, 46 (5%) children have required transplants, and 22 (2%) deaths have been reported to WHO.
Almost half (48%) of the probable cases have been reported from the WHO European Region (21 countries reporting 484 cases), including 272 cases (27% of global cases) from the United Kingdom of Great Britain and Northern Ireland (the UK) (Table 1, Figure 2). The second highest number of probable cases have been reported from the Region of the Americas (n=435, including 334 cases (33% of global cases) from the United States of America), followed by the Western Pacific Region (n=70), the South-East Asia Region (n=19) and Eastern Mediterranean Region (n=2). Seventeen countries are reporting more than five probable cases. The actual number of cases may be underestimated, in part due to the limited enhanced surveillance systems in place. The case count is expected to change as more information and verified data become available.
Figure 1. Distribution of probable cases of severe acute hepatitis of unknown aetiology in children by country, as of 8 July 2022 (n=1010), 5 PM CEST

Table 1. Distribution of probable cases of severe acute hepatitis of unknown aetiology in children by WHO Region since 1 October 2021, as of 8 July 2022, 5 PM CEST
| WHO RegionProbable casesCases requiring liver transplantsSARS-CoV-2 positive by PCR (Number of positive cases) Adenovirus positive by PCR⸸ (Number of positive cases)Adenovirus type 41 (Number of positive cases)DeathsAmericas43524189113Eastern Mediterranean20Not available1Not available1Europe4842254193302Southeast-Asia190Not availableNot availableNot available6Western Pacific7006600Cumulative*101046782093122 |
*The information included in this table contains data notified under IHR (2005), including from The European Surveillance System (TESSY) and official sources detected through event-based surveillance activities within the Public Health Intelligence process. Further information is presented in the Annex table.
⸸ Adenovirus positive in any specimen type (respiratory, urine, stool, whole blood, serum, other, or unknown specimen type)
Laboratory testing of cases
Based on the working case definition for probable cases (Box 1), laboratory testing has excluded hepatitis A-E viruses in these children. Pathogens like adenovirus and SARS-CoV-2 were detected by PCR in a number of the cases, although the data reported to WHO are incomplete.
Adenovirus continues to be the most frequently detected pathogen among cases with available data. In the European region, adenovirus was detected by PCR in 52% of cases (193/368) with available results (see Annex). In Japan, adenovirus was detected in 9% of cases (5/58) with known results. Due to limited adenovirus surveillance in most countries, it is challenging to assess whether these rates are higher than the expected rates in the population.
SARS-CoV-2 has been detected in a number of cases, however, data on serology results are limited. In the European region, SARS-CoV-2 was detected by PCR in 16% of cases (54/335) with available results (see Annex). Preliminary reports from the United States of America indicate that SARS-CoV-2 was detected in 8% of cases (15/197) with available results. In Japan, SARS-CoV-2 was also detected in 8% of cases (5/59) with available results. These figures may change as new data becomes available.
Most reported cases did not appear to be epidemiologically linked; however, epidemiologically linked cases have been reported in Scotland, and the Netherlands.
Box 1. WHO Working case definition of severe acute hepatitis of unknown aetiology

Epidemiological characteristics of cases
Of 571 probable cases (57% of all probable cases) for which data are available, there has been a decreasing trend in cases over the last month (Figure 2). However, this trend should be interpreted carefully as there are reporting delays and limited surveillance in many countries.
Figure 2. Epidemiological curve of probable cases of severe acute hepatitis of unknown aetiology with available data, by week, by WHO region, as of 8 July 2022 (n=571), 5 PM CEST

Note: Figure 2 includes cases for which dates of symptom onset, hospitalization, or notification were reported to WHO (n= 571). The date of symptom onset was used when available (n=384). If unavailable, the week of hospitalization (n=163), or the week of notification (n=24), was used.
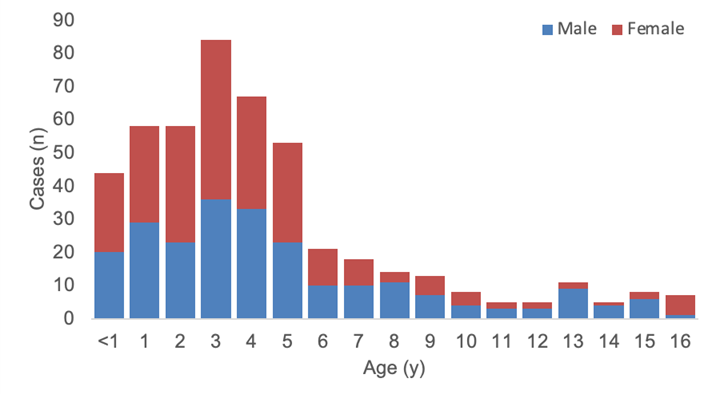
As of 8 July 2022, of 479 cases with information on gender and age, 48% are male (n=232), and the majority of cases (76%, n=364) are under six years of age (Figure 3).
Figure 3. Age and gender distribution of reported probable cases of severe acute hepatitis of unknown aetiology with available data, as of 8 July 2022 (n=479) 5 PM CEST
Out of 100 probable cases with available clinical data, the most commonly reported symptoms on presentation were nausea or vomiting (60% of cases), jaundice (53% of cases), general weakness (52% of cases) and abdominal pain (50% of cases).
Of all global cases with available data, a total of 167 cases (16% of all probable cases) had both date of symptom onset and date of hospitalization available. Among these, the median number of days between date of symptom onset and date of hospitalization was four days [interquartile range (IQR) 7].
Public health response
Epidemiological, clinical, laboratory, histopathological and toxicological investigations of the possible aetiology (or aetiologies) of the cases are underway by several national authorities, research networks, across different working groups in WHO and with partners. This includes detailed epidemiological investigations to identify common exposures, risk factors or links between cases.
On 11 July 2022, WHO launched a global online survey with an aim to estimate the incidence of severe acute hepatitis of unknown aetiology in 2022 compared to the previous five years, to understand where cases and liver transplants are occurring at higher-than-expected rates. WHO has shared the voluntary survey across nine global and regional networks of paediatric hepatologists and other specialist paediatricians working in major national units, requesting aggregated data as part of the global event investigation. Interim results of the survey will be made available publicly by WHO as soon as they are available.
The specific objectives of the survey are to:
- Assess whether there has been a recent increase or not in incidence of severe acute hepatitis of unknown aetiology (with and without acute liver failure) in children ≤16 years, including those requiring liver transplantation, in different countries and regions (number of cases in 2022 compared to 2017-2021)
- Assess any changes in the age distribution and severity of reported cases over time (2022 compared to 2017-2021).
Source: WHO

{kind=link}